- Home
- About the Journal
- Peer Review
- Editorial Board
- For Authors
- Reviewer Recognition
- Archive
- Contact
- Impressum
- EWG e.V.
Cite as: Archiv EuroMedica. 2022. 12; 4: e1. DOI 10.35630/2199-885X/2022/12/4.9
Breast cancer (BC) poses a serious threat to the health and life of women of all ages all over the globe. The most important task in breast cancer diagnosis is to identify the disease at an early stage. Therefore, there is a need for annual examination, primarily for women with risk factors. So, the current trend requires development and implementation of new approaches to early detection and timely treatment of BC. Among the list of new technologies for early screening is development of a portable in-house "smart" mammograph T-screen. Our clinical studies involved 198 women who used the device and confirmed its high sensitivity and specificity. The proposed method is absolutely harmless, informative, it can be used any number of times, regardless of age and pregnancy. Such data on high safety allow using T-screen widely for preventive purposes, both in early diagnosis and to detect a risk group of breast cancer in women. The methodology for using the device that we propose is simple and accessible to any user.
Keywords: breast cancer, prevention, population screening, screening mammograph
Breast cancer (BC) takes a leading place in the structure of oncological diseases in most countries of the world. According to the World Health Organization (WHO) and the cancer database GLOBOCAN, 2.3 million women received this diagnosis in 2020. The average annual growth rate for ten years was 1.97%. The number of healthy life years lost (DALYs) for women with BC worldwide exceeded those for any other type of cancer. The vast majority of deaths from breast cancer are associated with late diagnosis, metastasis and recurrence [2, 3, 5, 12, 16].
Therefore, demand for modern inexpensive and accessible tools determining the risk of developing oncology, and for screening methods to rank the population flows of women in order to identify BC risk groups at an early stage, when treatment allows achieving stable recovery in 90 - 95% of patients, has sharply increased [1, 4, 8, 10, 14, 15].
A good commercial potential of developments for screening has attracted the attention of scientists around the world. In the field of early detection of breast cancer, creative teams from different countries are making their experiments today. Thus, a team from Poland proposed a device for early screening BRASTER PRO, which is based on the principles of thermography. Also, for early diagnosis of neoplasms, UE Life Sciences, Philadelphia, PA developed the device iBrest Exam using the capacitive sensing technology based on the modulus of elasticity. The Chinese developers, in their turn, proposed the mammograph COZING-XS01 for local use, which is based on infrared sensing technology. The practical use of the products of this group showed similarity of technical and clinical indicators, including sensitivity and specificity (on average, no worse than 80%), the time of examination (from 3 minutes to 15 minutes) and the ability to detect a tumor from 3 mm in size. Today, such technical advances make screening quite competitive compared to conventional research methods such as X-ray and ultrasound [6, 13].
The handheld portable mammograph T-screen (ООО "Intellectual Program Systems” Saint Petersburg, Russia) designed for home use, which allows self-examination independently outside a medical institution, became a significant addition to the group of screening devices [7, 9, 10].
The principle of T-screen operation is based on the electrical impedance method with assessment of electrical resistance distribution on the surface of breasts, which depends on violations of the structure of the internal tissues of the organ. It is known that malignant tissue has a higher conductivity than healthy tissue. The tumor is found as the areas with abnormal conductivity values [11, 13].
Upon completion of the study, we have a comprehensive presentation of the results of examination in form of text and images, both on the screen of a smartphone and a tablet. All areas of the breast are examined, taking into account its size. The examination is carried out in quadrants. The application for T-screen is available on smartphones or tablets with Android 4.0 Windows and above.
The device belongs to the class of "smart" devices capable of detecting neoplasms, fibrocystic disease, mastitis, physiological involution, etc. using original software. The software of T-screen allows, with the use of artificial intelligence methods, determining risk factors – a highly sensitive and specific parameter sensitive to neoplasms in the mammary gland, detecting fast-growing fibroadenomas, timely detection of which at stages 1 and 2-A can prevent the disease in 90 - 95% of cases. It is also possible to provide quantitative assessment of the risk of neoplasms in digital form (risk factor, BIRADS level (Breast Imaging-Reporting and Data System) [9, 10, 13].
The benefits of using T-screen include:
The above positive features of the technology were confirmed in course of an experimental clinical multicenter study to evaluate effectiveness of the device. It involved 198 women; the average age was 43.2 ± 4.5 years. Observation was carried out in the preoperative period of BC treatment. The diagnosis of oncological disease was established according to the current recommendations "Breast Cancer" [9, 10].
All patients were examined using a handheld mammograph and the obtained data were compared with the results of a mammological study obtained using full-field digital mammography (Siemens mammograph for Full Field Digital Mammography FFDM) with a second-generation CsI-based detector, which was carried out in compliance with GOST R 50267.45-99 (IEC 60601-2-45-98) "Medical electrical products. Part 2", as well as with the results of ultrasound and the conclusion of doctors [9, 10].
For the convenience of using a mammograph, we have developed a method for performing a study with its help. The examination was performed in a supine position with maximum comparison and correct orientation of the electrode array of the impedance mammograph (according to the instructions) with the skin surface of the breast. The sensor was applied to the mammary gland sequentially according to the scheme we proposed. So, first the sensor was placed on the area of the nipple and areola, then sequentially on each of the four sectors of the breast, first on the lateral, and then on the medial areas. Thus, five measurements of each breast are carried out:
During the examination of the patients, it was revealed that 6.4% had no changes in the mammary gland; in 55.1% of cases, a malignant neoplasm was diagnosed, with 39.5% at the first stage, 48.8% at the second, 11.6% at the third, 38.5% had benign breast changes.Below is an example of a picture of mammary glands impedance in patients with stage 2 NEO obtained using a handheld mammograph T-screen (Figure 1).
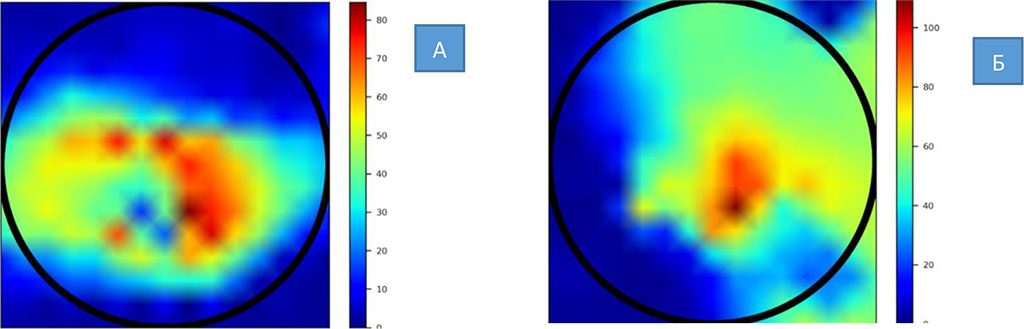
Figure
1. A picture of breast impedance in patients with stage 2 NEO
a
– diagnosis – invasive cancer of nonspecific type, location –
upper outer quadrant;
b
– diagnosis – nodular cancer, location – upper inner quadrant,
after 8 courses of PCT.
As a result of the study, it was noted that:
According to the results of the study, results were obtained on the lesion of the right breast in 52.6% of cases; the left in 30.8% of cases; bilateral - in 11.5% of patients. The data obtained are comparable with the results of mammography, ultrasound and the BIRADS (Breast Imaging Reporting and Data System) system. The BIRADS system is a system for interpreting and logging breast imaging, where category 0 - requires additional imaging, 1 - no changes, 2 – benign changes, 3 - probably benign changes, 4 – suspected cancer, 5 – characteristic of cancer, 6 – cancer confirmed by biopsy. Statistical studies (ROC analysis) have shown sufficient "sensitivity" and "specificity" for the screening method - no worse than 0.75 [9, 10].
At the same time, mass screening has always been and remains a costly medical event, sometimes beyond the reach of certain population groups. When conducting mass screening examinations, a way out can be found in replacement of heavy medical equipment: X-ray, MRI and ultrasound, with handheld, smart devices that do not have radiation exposure. To confirm this hypothesis, we compared the results of studies of the state of breast tissue using an X-ray mammograph and a handheld screening device T-screen. Creating a "smart" mammograph, we fulfilled the task that consisted in meeting the needs of main recipients of the screening service – women. Their main wish was the quality, reliability, ease of use, time of examination, comfort and affordability of mammary glands examination [6, 7, 9, 10].
The following criteria were taken as baseline data:
The comparison was carried out on the examples of two in-house models of X-ray mammographs that are widely available on the Russian healthcare market – mammographs Philips MicroDose and Hologic Lorad Selena. The first device, apart from the standard CC-craniocaudal and MLO-mediolateral projections, is able to additionally perform axillary non-invasive spectral imaging scanning projections. For a clinical device, such functionality is undoubtedly necessary. However, for primary mass screening, it may be redundant. The mammograph Hologic Lorad Selena provides a field of view of 24 x 29 cm or 170 degrees in a single exposure. Due to improvement of technology, it is able to catch neoplasms of 0.05 cm in size. Such accuracy is clearly important for a clinical device, but it is redundant for screening. It is important to note that with each new version of devices, they become more functional, thereby moving further and further away from the goals and objectives of screening [13].
The characteristics of X-ray and bioimpedance mammographs, both required and provided, are clearly presented in Figure 2 [7]:
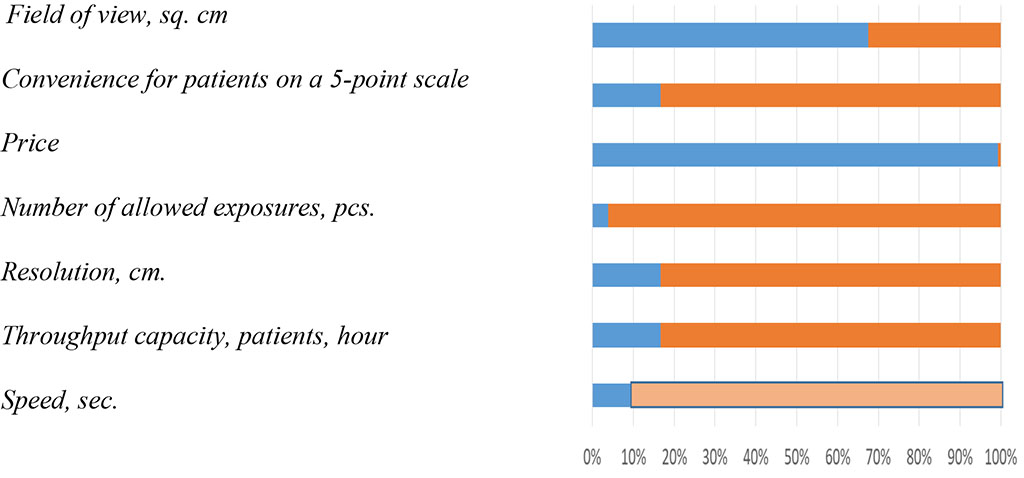
X-ray mammograph Bioimpedance mammograph
The mammograph T-screen is shown in Figure 3.
The graph shows that the bioimpedance technology almost fully meets the requirements for population screening, the key task of which is to identify neoplasms at a specific growth point in time and follow the dynamics (positive or negative) of further neoplasm development. Based on the results of dynamic observation, the patient herself will be able to determine the need for additional examination and choose the option of her future preventive or therapeutic route.

Figure 3. The mammograph T-screen
Thus, there is a solution to the problem of prophylaxis, which ensures healthy lifestyle. Inferior in terms of functionality compared to X-ray, this technology compensates for this with its accessibility in terms of comfort and convenience, involving the widest segments of the population in the screening pool, regardless of their place of residence and distance from the medical organization. Low cost allows purchasing the device in the family, use it for women of all ages. The cloud filling of the smart device will warn in time about possible threats to health. Having received a color image on a smartphone, the doctor, in turn, will be able to plan further therapeutic tactics, reducing time losses to a minimum.

|
||